
Robotic Surgical Videos for Complex Abdominal Surgery
These operative videos demonstrate robotic pancreatic surgery, robotic liver surgery, and other advanced hepatopancreatobiliary (HPB) and gastrointestinal cancer procedures performed using minimally invasive robotic techniques.
Understanding Robotic Surgical Oncology
Watch educational videos demonstrating how advanced robotic techniques are applied to complex cancer operations.
This surgical video library provides an inside look at how robotic-assisted surgery is used in the treatment of pancreatic, liver, bile duct, gastric, esophageal, and other complex abdominal cancers. These procedures fall within the field of hepatopancreatobiliary (HPB) and gastrointestinal surgical oncology, where millimeters often separate tumors from critical vascular and biliary structures.
Robotic platforms provide enhanced three-dimensional visualization, refined instrument articulation, and improved precision within confined anatomical spaces. These capabilities are particularly valuable in technically demanding operations such as robotic pancreatic surgery, robotic liver surgery, and complex minimally invasive gastrointestinal cancer procedures.
For appropriately selected patients, robotic techniques may allow for smaller incisions, meticulous tissue handling, reduced postoperative discomfort, shorter hospital stays, and a more efficient recovery — while maintaining rigorous oncologic standards including complete tumor removal and appropriate lymph node evaluation.
These videos are designed to help patients, families, and referring physicians better understand how robotic surgical oncology techniques are applied in real clinical cases, and why a robotic approach may be recommended as part of an individualized treatment strategy.
Our goal is to integrate advanced surgical technology with disciplined oncologic technique and thoughtful, patient-centered care. Dr. Krampitz is recognized as a Master Surgeon in Robotic Surgery by the Surgical Review Corporation, an independent organization that evaluates surgeon experience, outcomes, and adherence to established quality benchmarks in robotic surgery. This commitment allows patients to move forward with clarity, confidence, and a treatment plan grounded in both innovation and experience.
These cases reflect real operative experiences in robotic hepatopancreatobiliary and gastrointestinal surgical oncology and are presented to support education for patients, trainees, and referring physicians.
For physicians seeking referral information or multidisciplinary collaboration, please visit the For Referring Physicians page.
Selected Robotic Operative Demonstrations
The following cases include robotic pancreatic resection, robotic liver resection, biliary surgery, upper gastrointestinal cancer surgery, and colorectal cancer surgery.
These demonstrations are intended for educational purposes and highlight key operative principles including oncologic dissection, vascular control, intraoperative ultrasound guidance, and minimally invasive reconstruction.
Robotic Hepatopancreatobiliary (HPB) Surgery
Hepatopancreatobiliary (HPB) surgery involves the treatment of complex diseases affecting the pancreas, liver, and bile ducts. These operations are among the most technically demanding procedures in abdominal surgery, often requiring meticulous dissection near major blood vessels and delicate biliary structures.
Robotic surgical platforms can enhance visualization and instrument precision in these confined anatomical spaces. High-definition three-dimensional optics and articulating instruments allow refined movements that support careful tumor dissection, vascular preservation, and precise tissue handling.
In appropriately selected patients, robotic techniques may be applied to procedures such as robotic liver surgery, robotic pancreatic surgery, and complex biliary operations, while maintaining the fundamental oncologic principles of complete tumor removal, appropriate lymph node assessment, and multidisciplinary cancer care.
The videos in this library include selected operative demonstrations from robotic HPB and gastrointestinal cancer surgery, illustrating how advanced minimally invasive techniques are integrated with disciplined surgical oncology practice.
Robotic Pancreatic Surgery
Robotic pancreatic surgery may be used for selected pancreatic tumors, including pancreatic cancer and pancreatic neuroendocrine tumors. Robotic platforms provide improved visualization and articulation in the confined retroperitoneal space surrounding the pancreas.

Robotic Liver Surgery for Liver Tumors and Liver Metastases
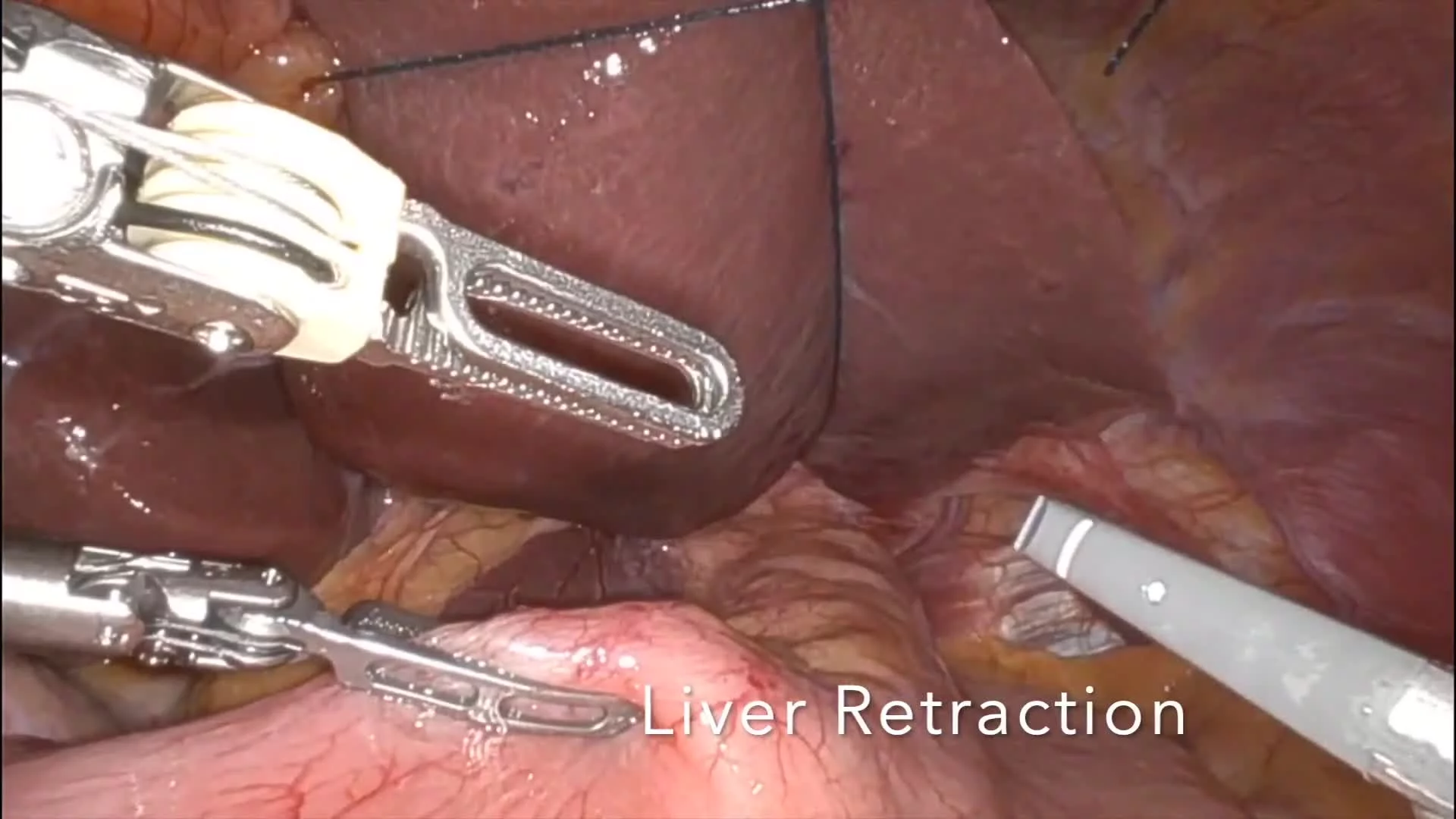
Robotic liver surgery can be applied to selected patients with liver tumors and liver metastases. High-definition three-dimensional visualization and precise instrument articulation support meticulous dissection and ultrasound-guided tumor localization during minimally invasive hepatobiliary procedures.
Robotic Biliary Surgery
Robotic techniques can also be applied to complex biliary procedures involving the bile ducts and gallbladder, including operations for cholangiocarcinoma and other hepatobiliary conditions requiring precise dissection near critical vascular structures.

Robotic Upper Gastrointestinal Cancer Surgery
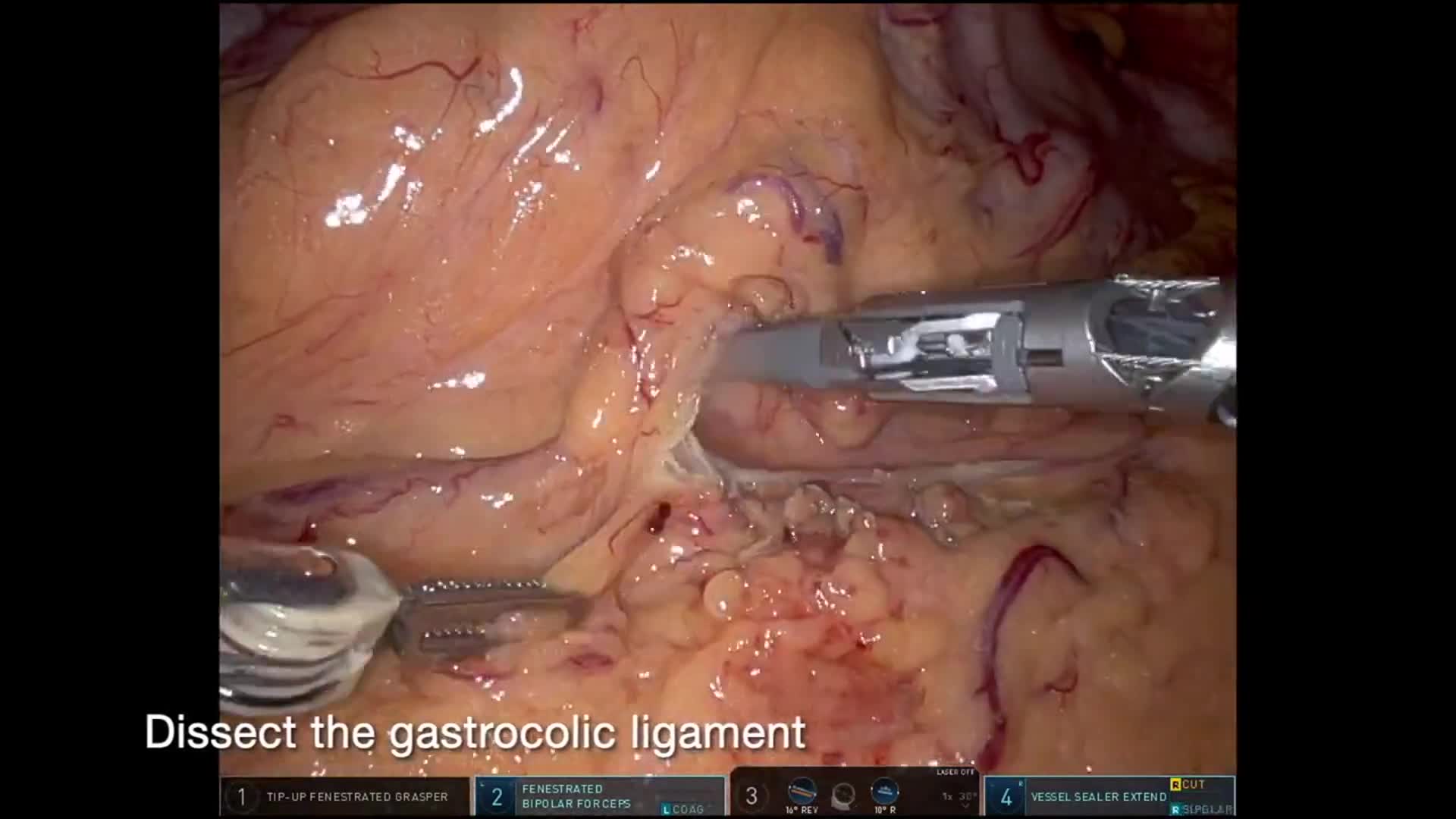
Robotic surgical platforms can enhance visualization and precision during operations involving the stomach, esophagus, small intestine, colon, and other complex abdominal organs. These procedures often require meticulous dissection in confined anatomical spaces, careful preservation of vascular structures, and precise reconstruction.
In appropriately selected patients, robotic techniques may be applied to gastric cancer surgery, esophageal surgery, colorectal cancer surgery, neuroendocrine tumor resection, and other complex abdominal oncologic procedures. High-definition three-dimensional visualization and articulating instruments can facilitate refined dissection and reconstruction while maintaining strict oncologic principles.
The following operative videos demonstrate selected cases of robotic upper gastrointestinal and complex abdominal oncologic surgery, illustrating how minimally invasive techniques are integrated with disciplined surgical oncology practice.

Robotic Colorectal Cancer Surgery
Robotic platforms can enhance visualization and precision during surgery for colon and rectal cancers, particularly in anatomically confined regions such as the deep pelvis. High-definition three-dimensional optics and articulating instruments allow refined dissection around critical vascular and autonomic structures while supporting meticulous oncologic technique.
In appropriately selected patients, robotic techniques may be used for procedures such as right hemicolectomy, sigmoid colectomy, and low anterior resection. These approaches allow precise vascular ligation, oncologic lymphadenectomy, and intracorporeal reconstruction while maintaining established principles of colorectal cancer surgery.
The following operative videos demonstrate selected cases of robotic colorectal cancer surgery, illustrating how minimally invasive techniques are integrated with disciplined surgical oncology practice.
Robotic Surgical Oncology in the San Francisco Bay Area
Dr. Geoffrey W. Krampitz is a fellowship-trained robotic surgical oncologist specializing in pancreatic cancer surgery, liver tumor surgery, bile duct cancer surgery, and complex gastrointestinal cancers. His practice provides advanced minimally invasive and robotic surgery for hepatopancreatobiliary (HPB) and gastrointestinal malignancies at Sutter Medical Center, Sacramento and Sutter Roseville Medical Center, serving patients throughout Northern California.
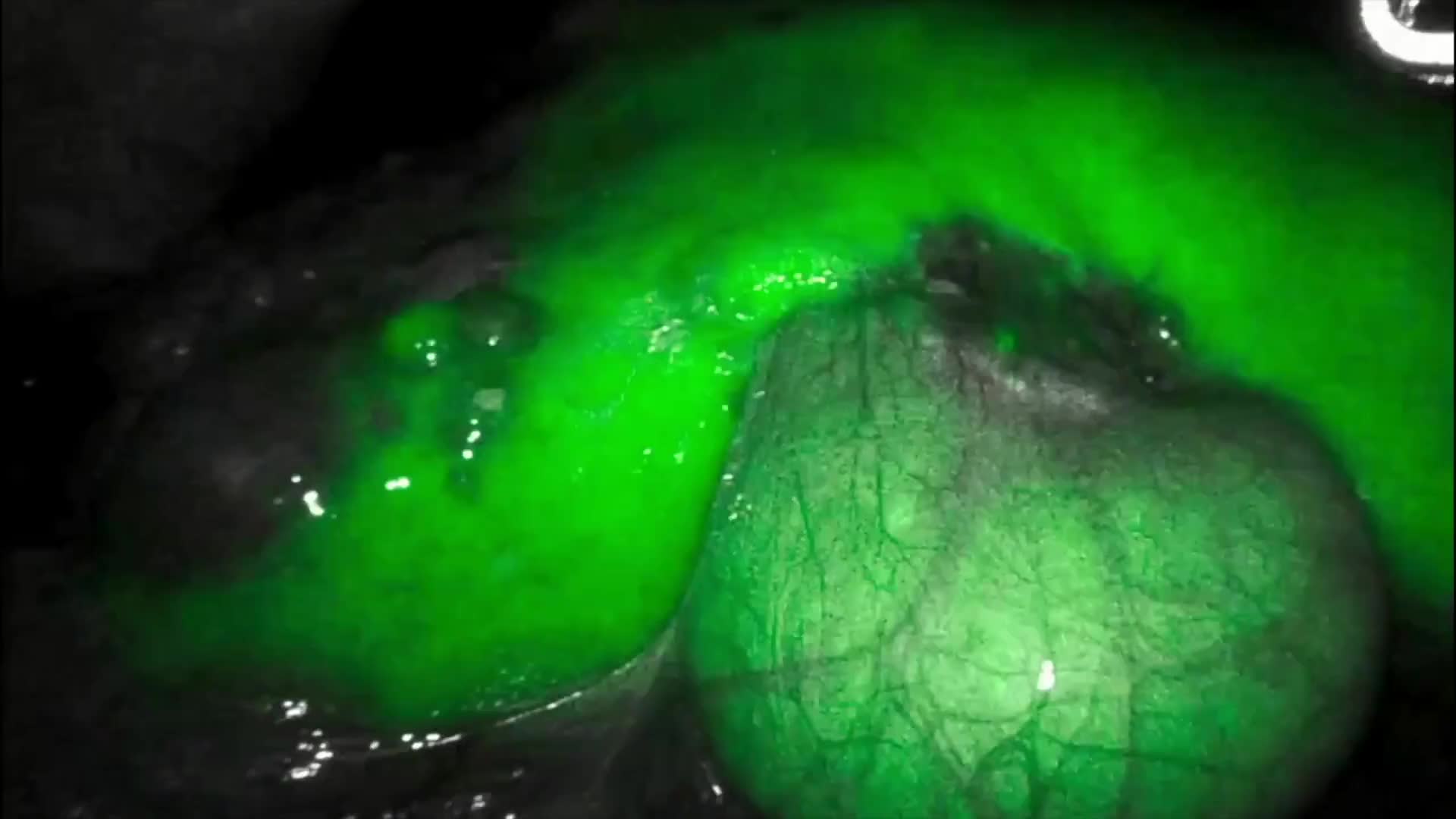
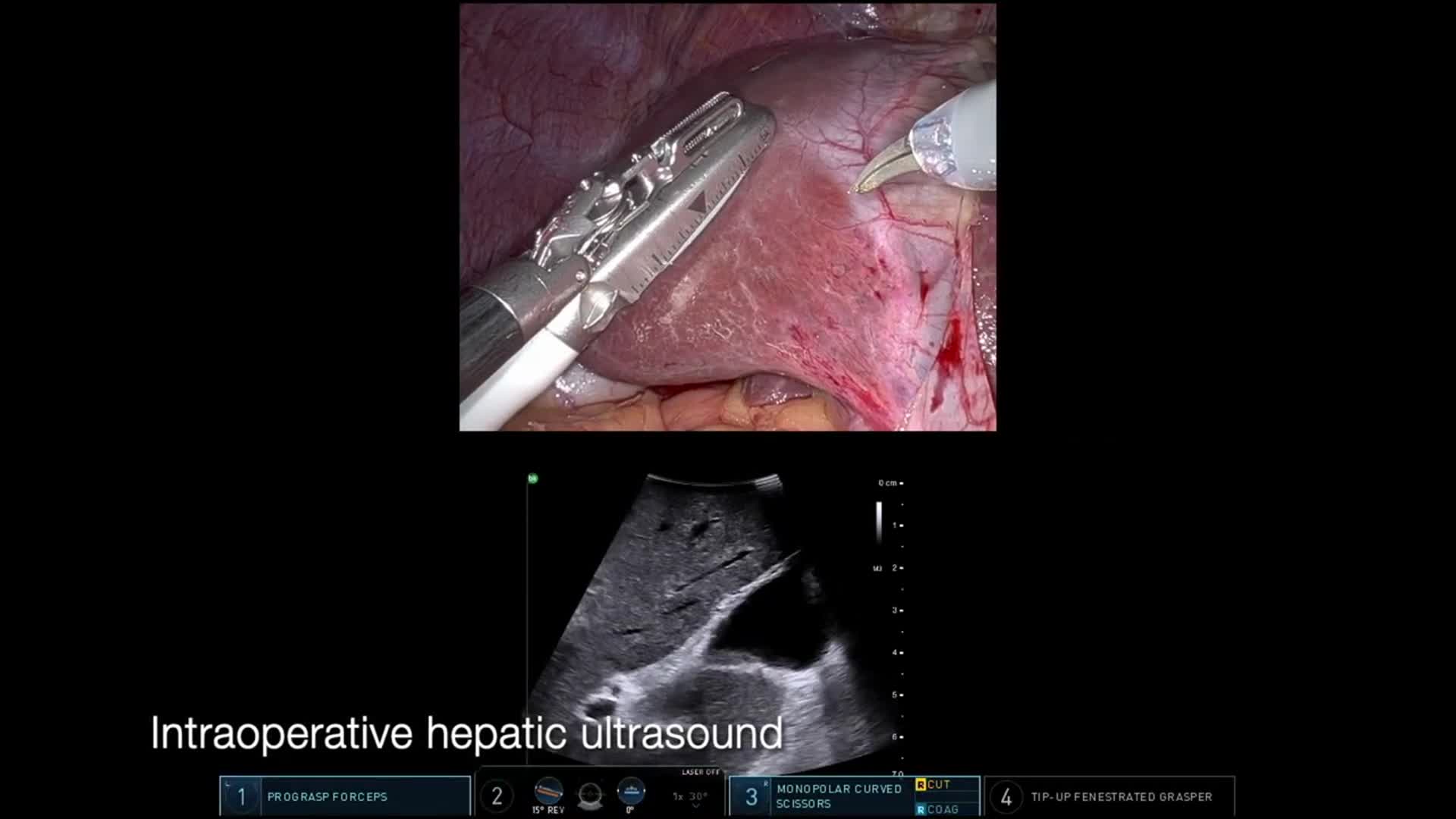
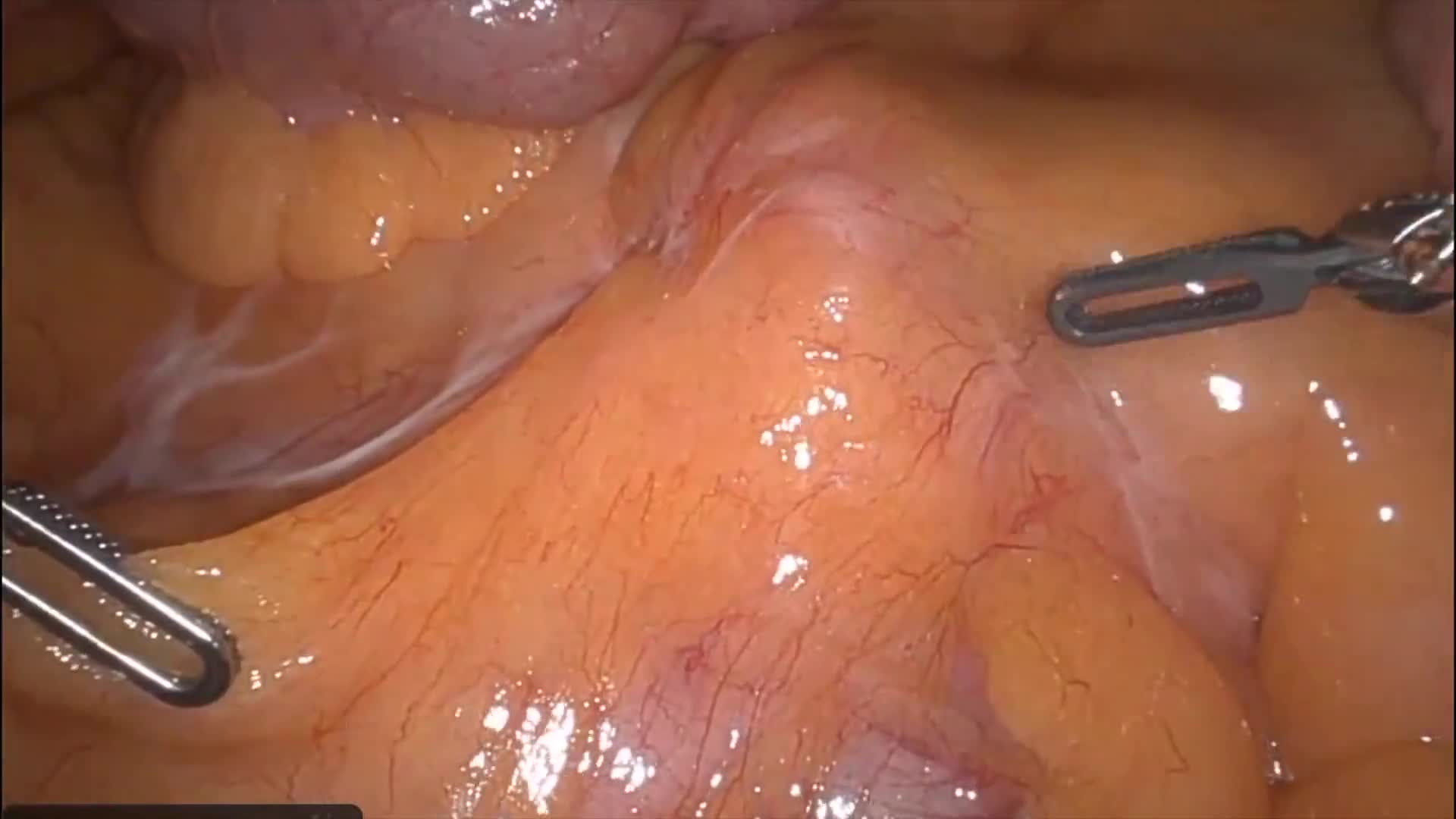
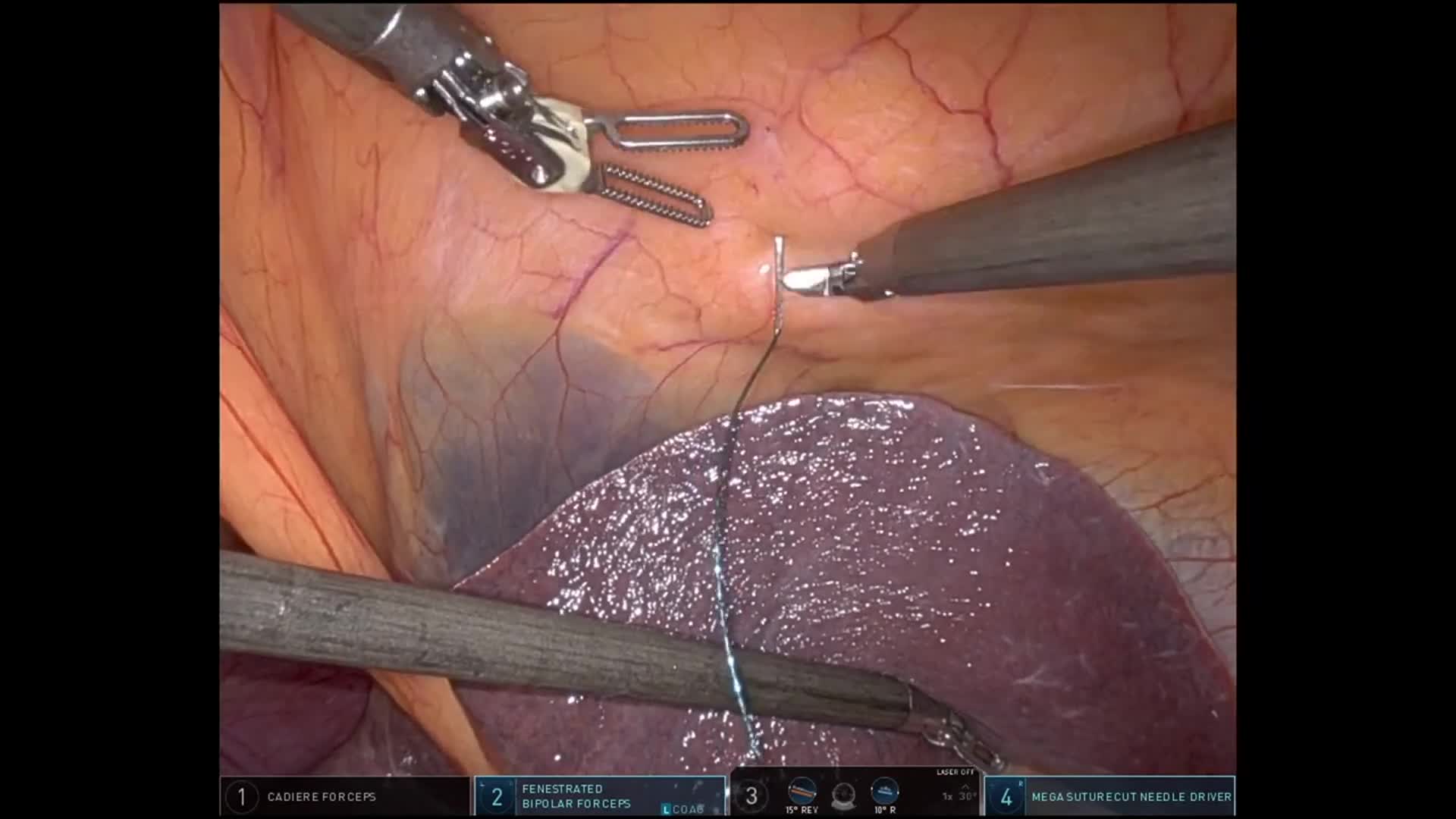
Robotic enucleation of a pancreatic neuroendocrine tumor with lymphadenectomy after prior ileal NET resection, demonstrating ultrasound-guided tumor localization and suprapancreatic dissection.
This case demonstrates robotic enucleation of a pancreatic neuroendocrine tumor with regional lymphadenectomyin a patient previously treated for an ileal neuroendocrine tumor.
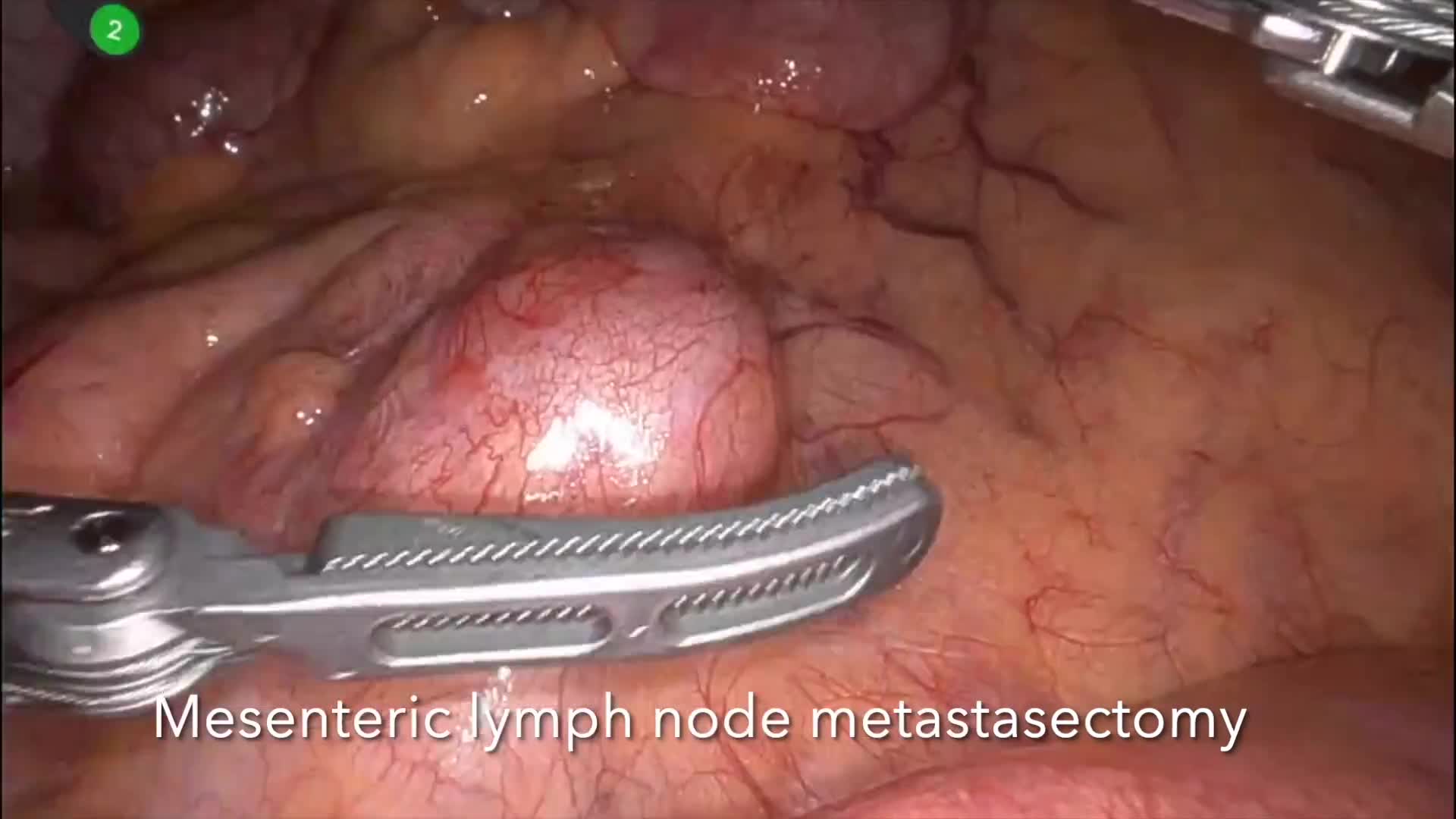
The patient initially presented with small bowel obstruction, and workup revealed a 1.7 cm well-differentiated ileal neuroendocrine tumor (WHO grade 1, Ki-67 <3%). He underwent laparoscopic small bowel resection, with pathology demonstrating pT3 pN1 disease with two of three regional lymph nodes involved.
Subsequent staging with DOTATATE PET/CT demonstrated intense radiotracer uptake in two nodular structures posterior to the pancreatic neck within the peripancreatic/gastrohepatic ligament region. Although initially interpreted as possible nonregional nodal metastases, the imaging characteristics and anatomic location also raised the possibility of a primary intrapancreatic neuroendocrine tumor.
Given the limited distribution of disease and the diagnostic uncertainty, surgical exploration was recommended.
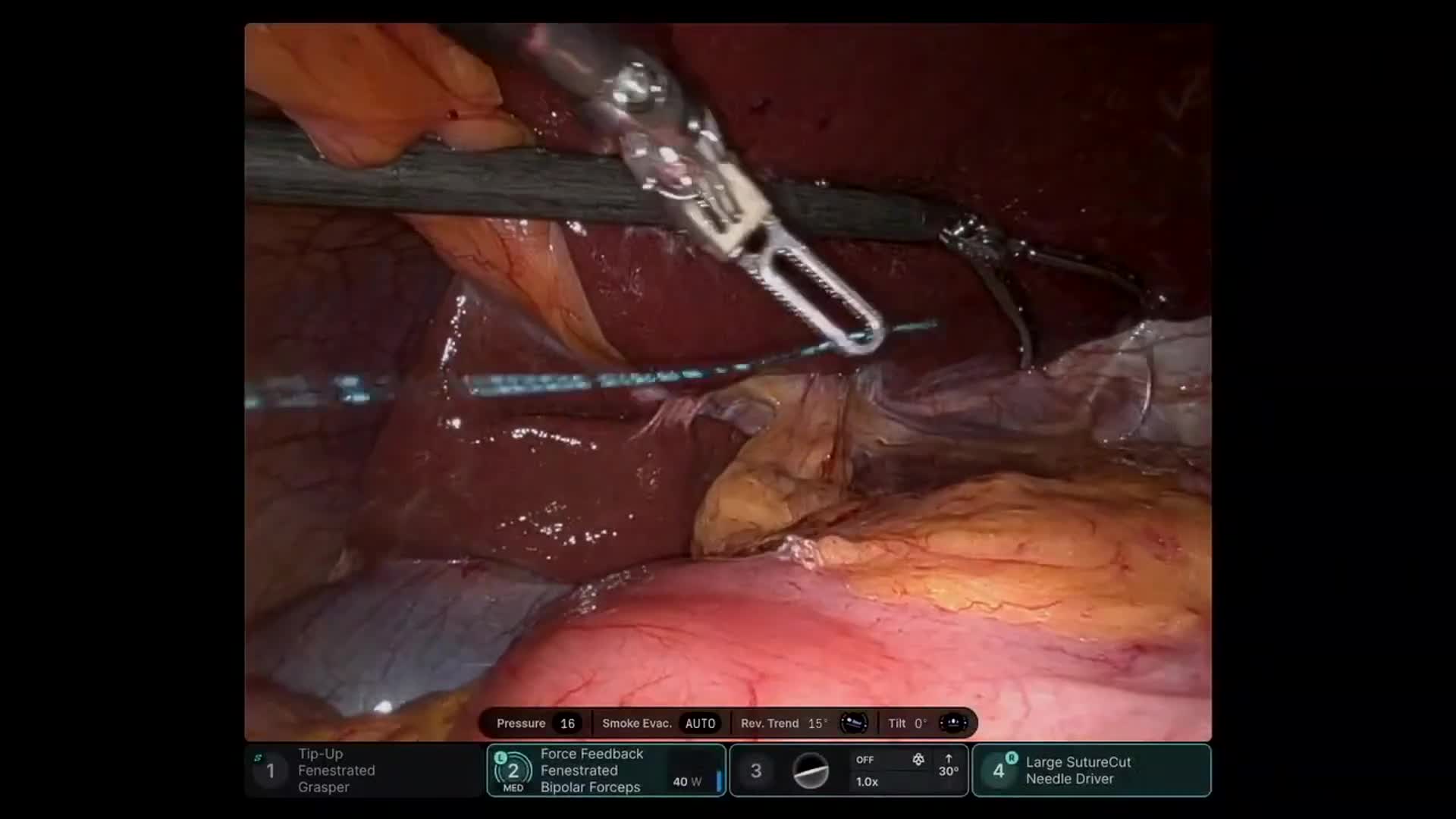
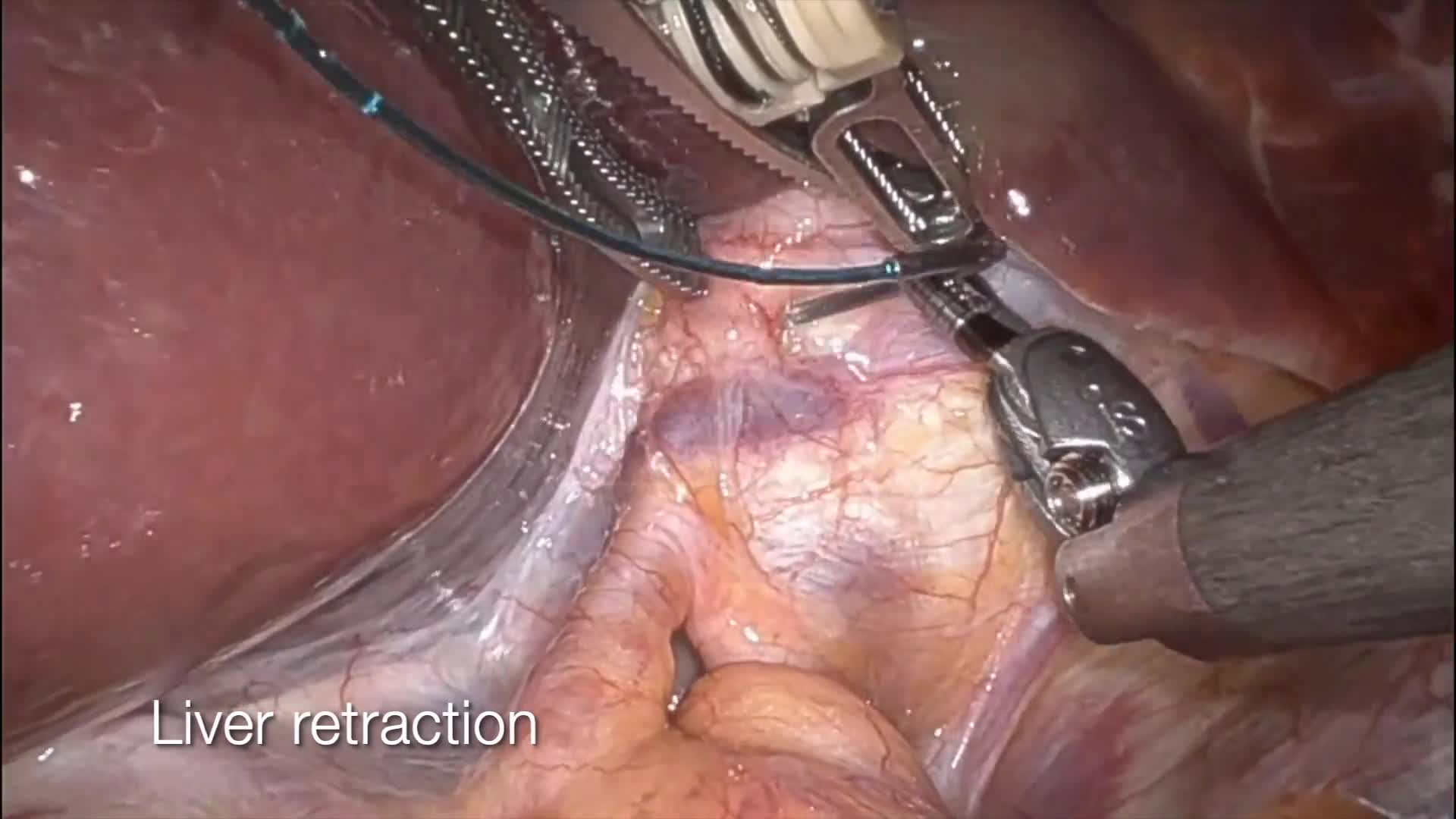
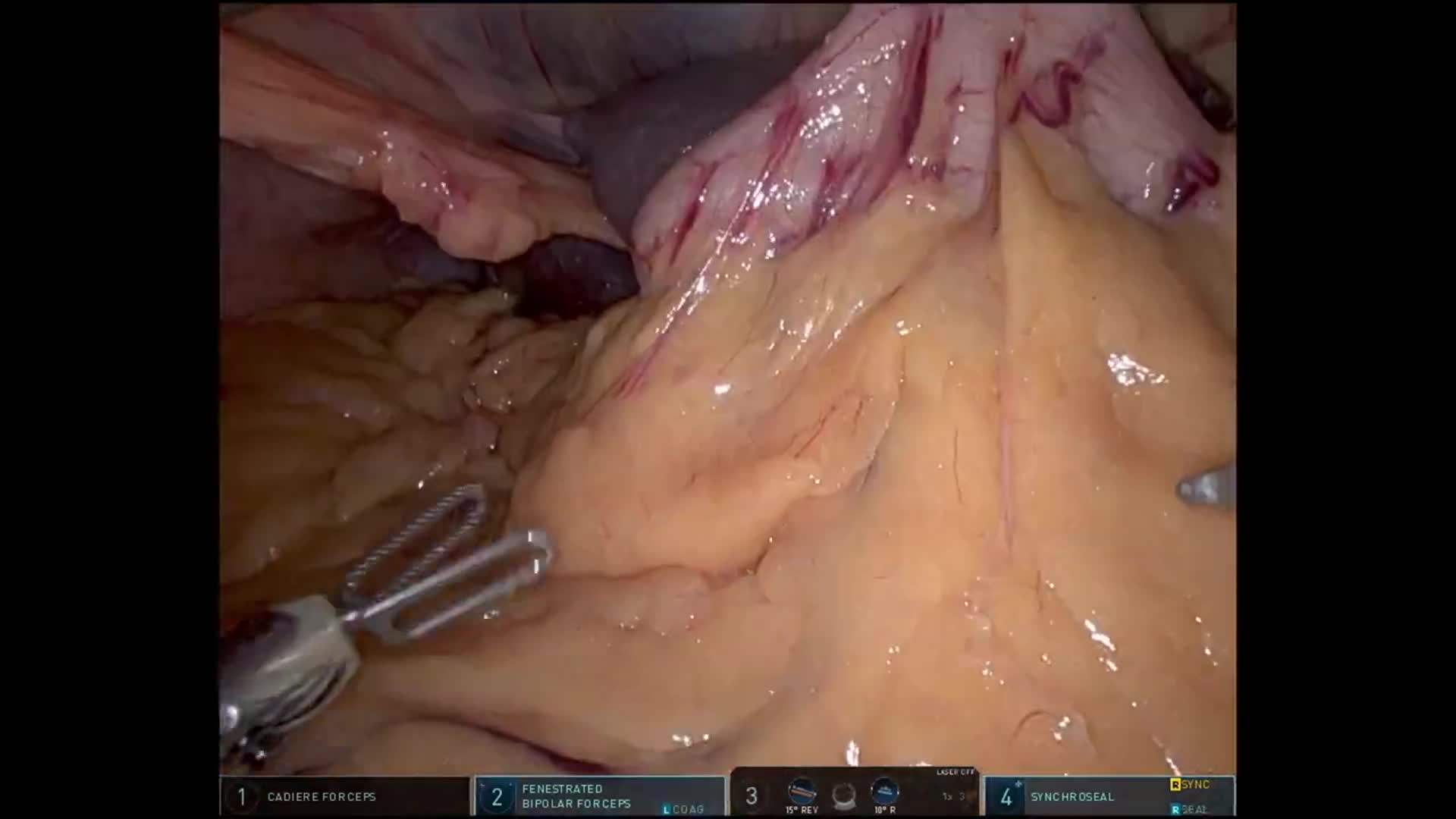
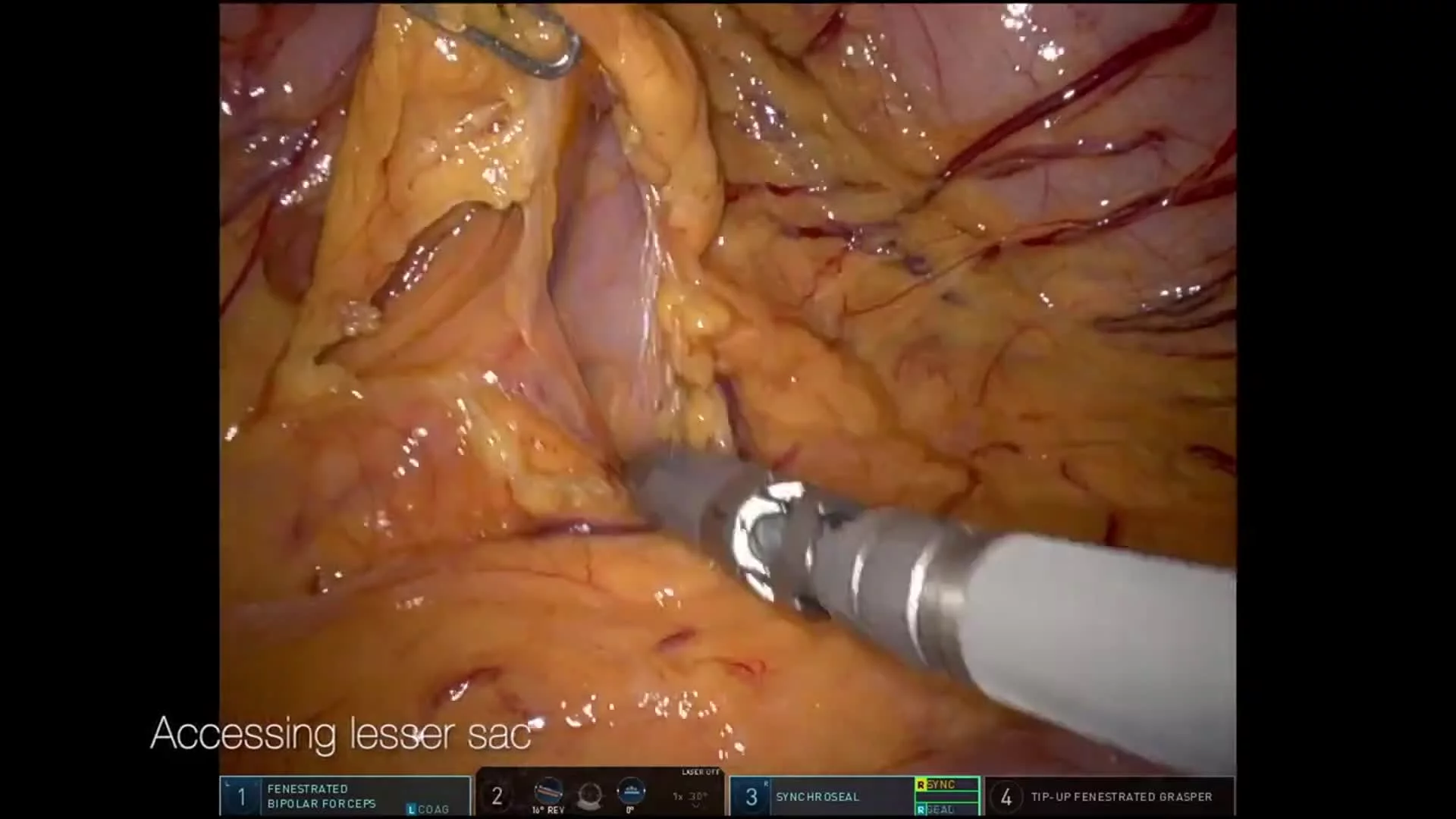
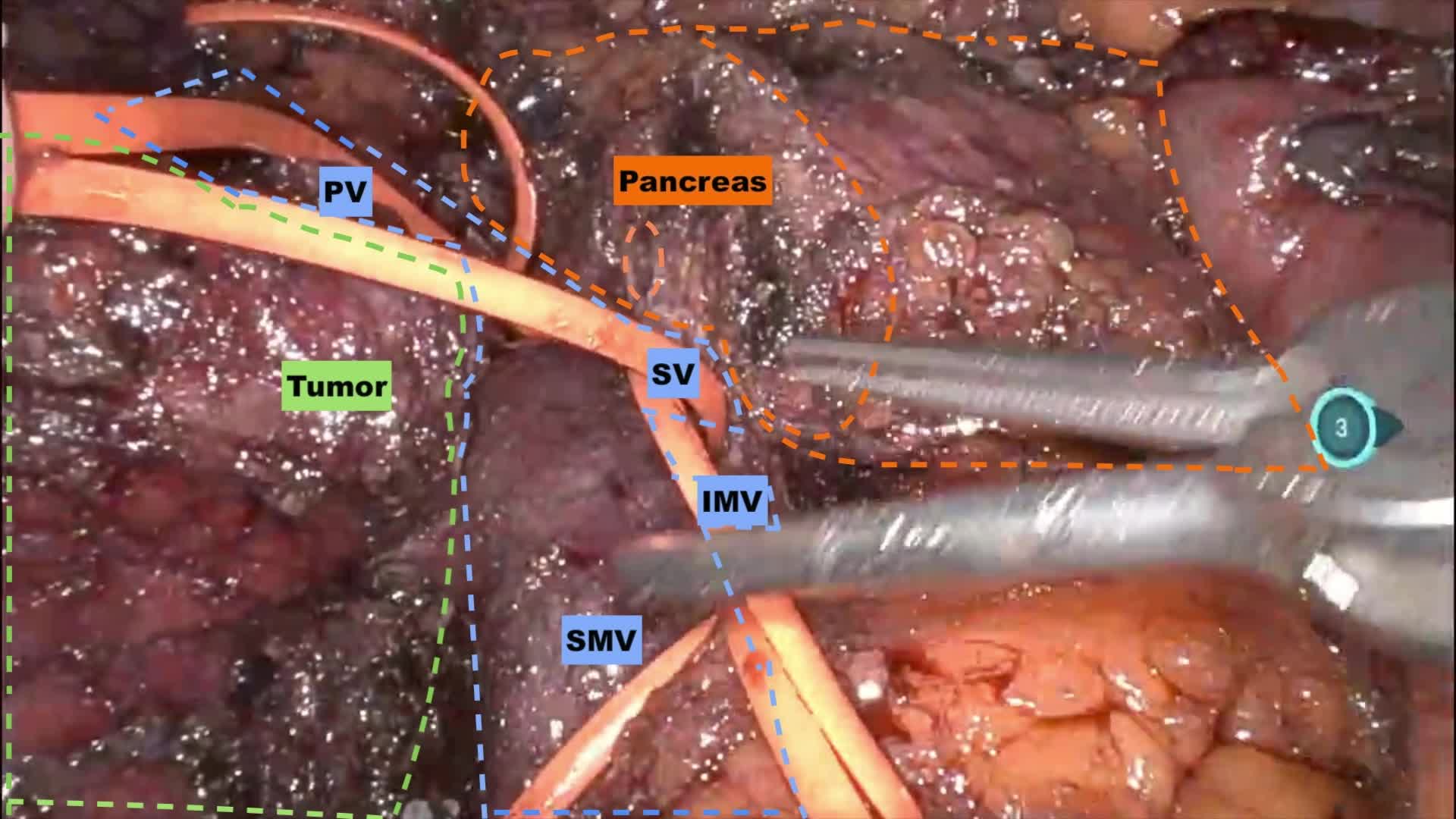
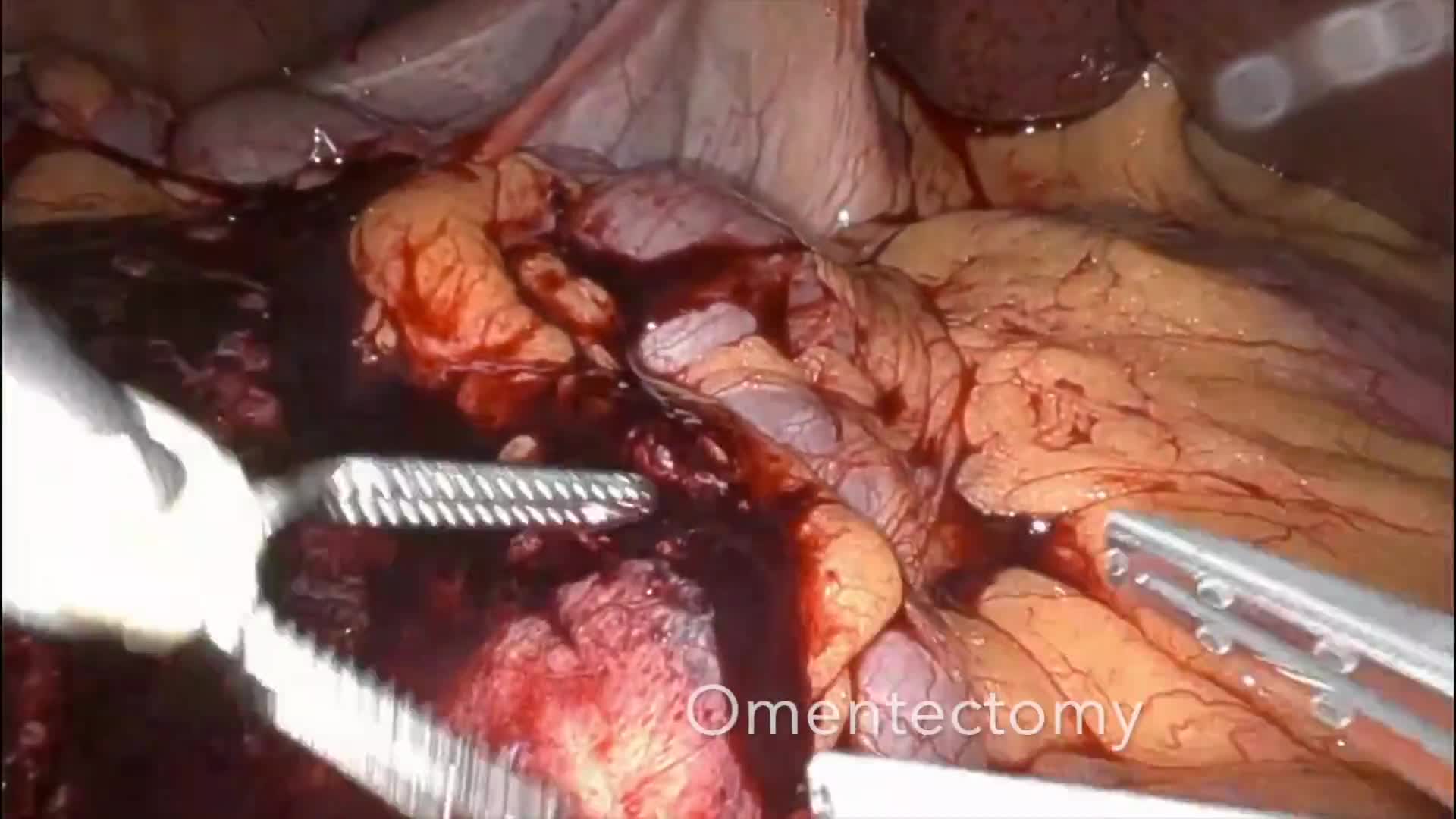
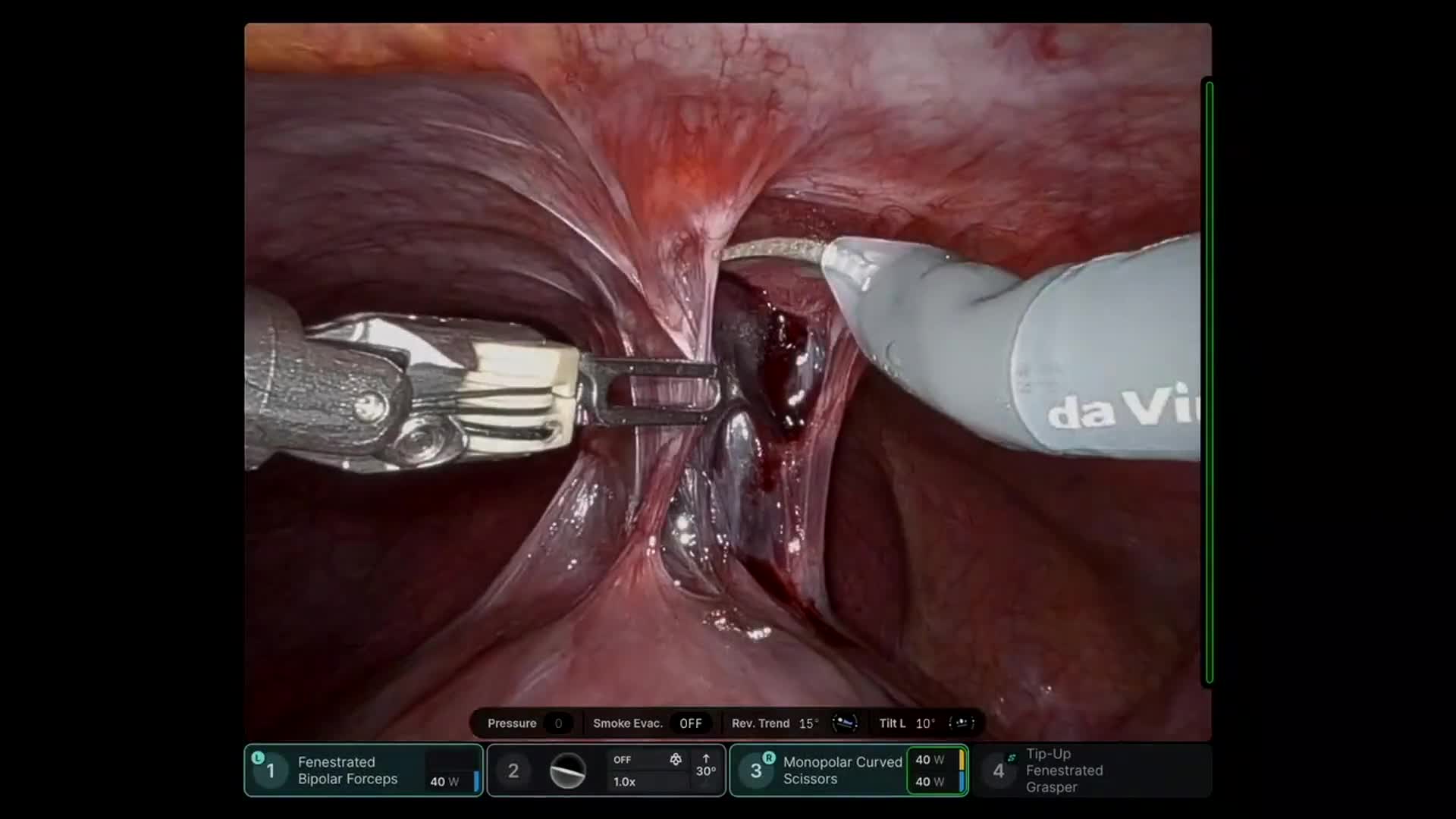
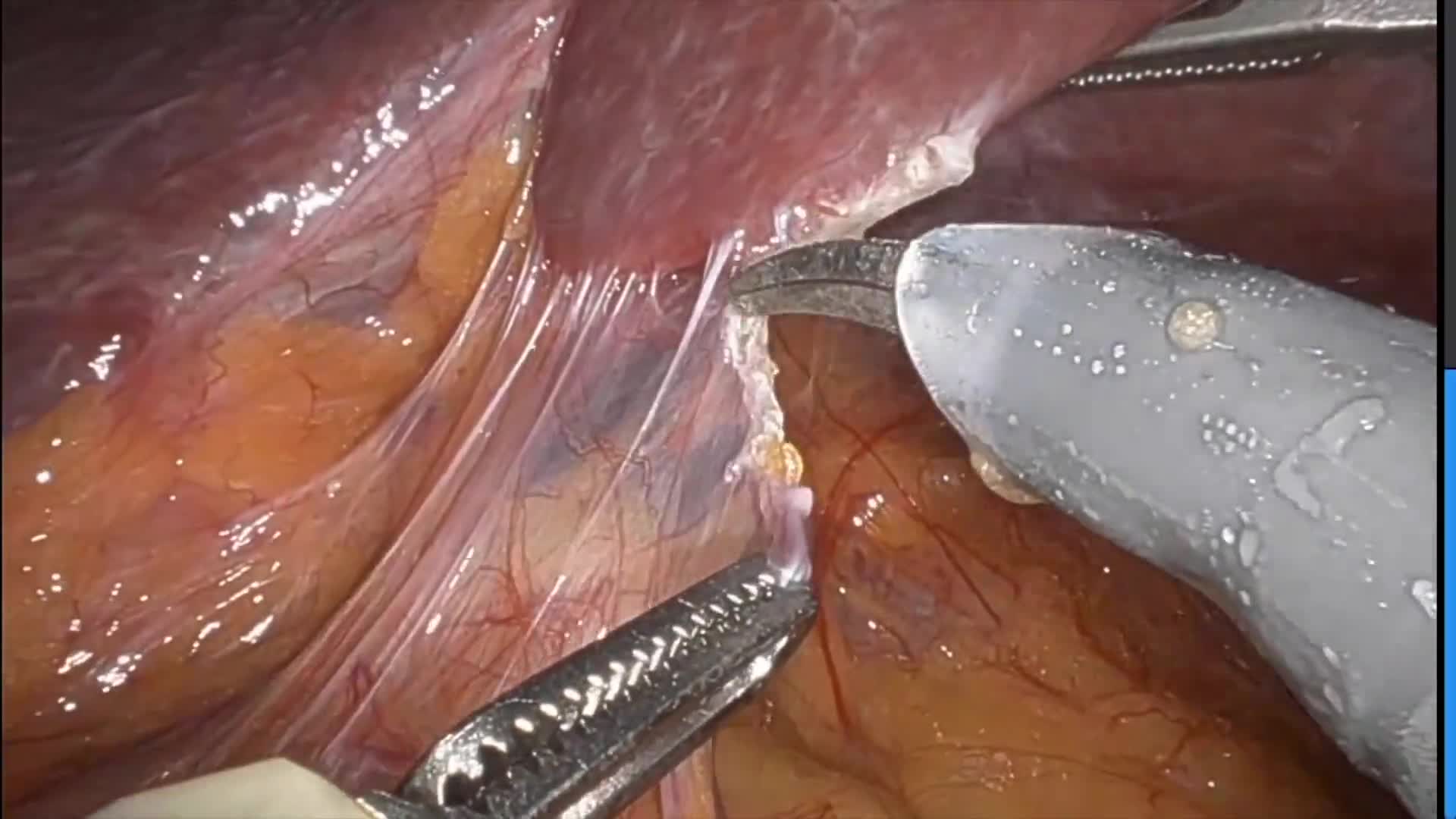
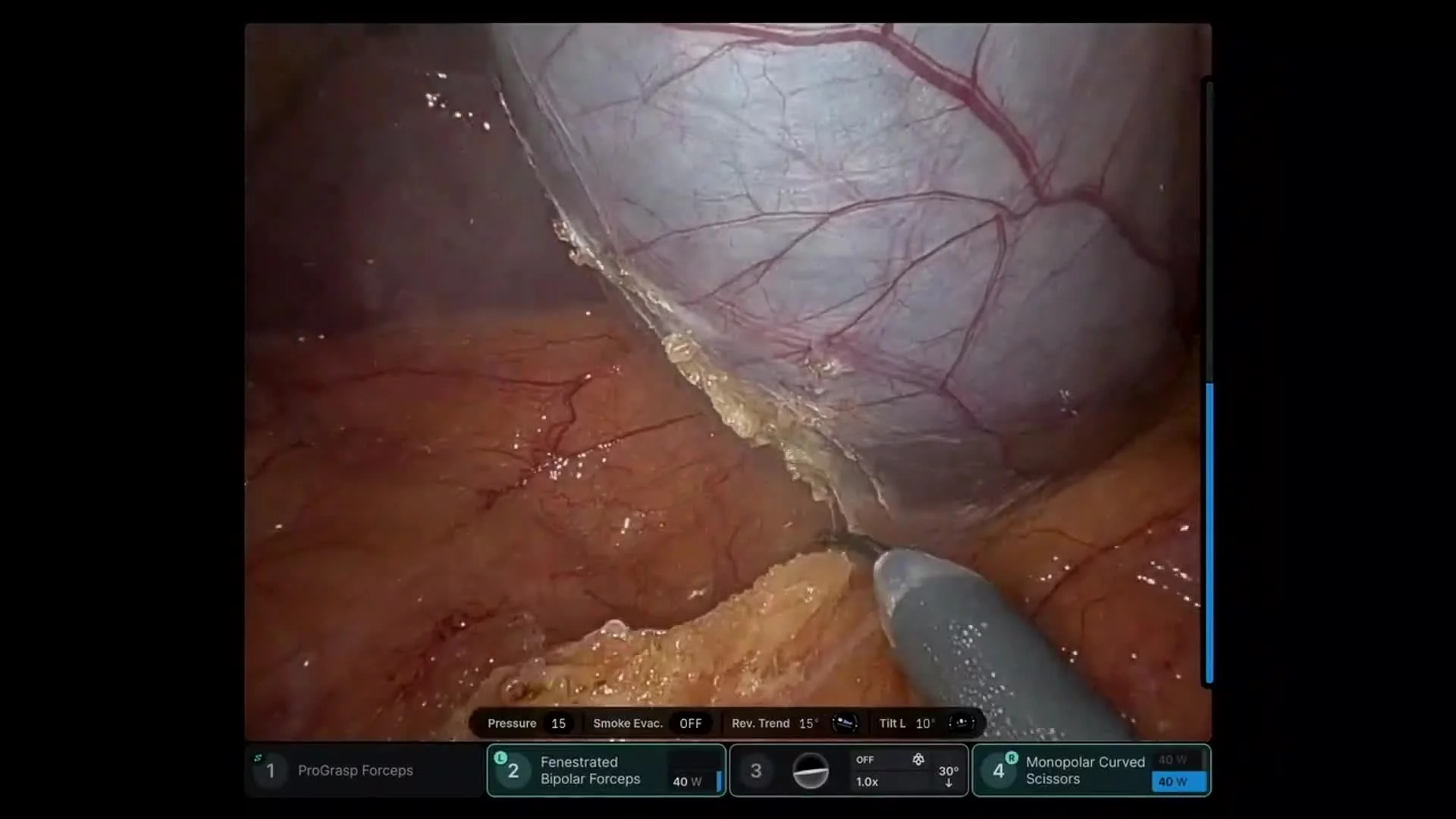
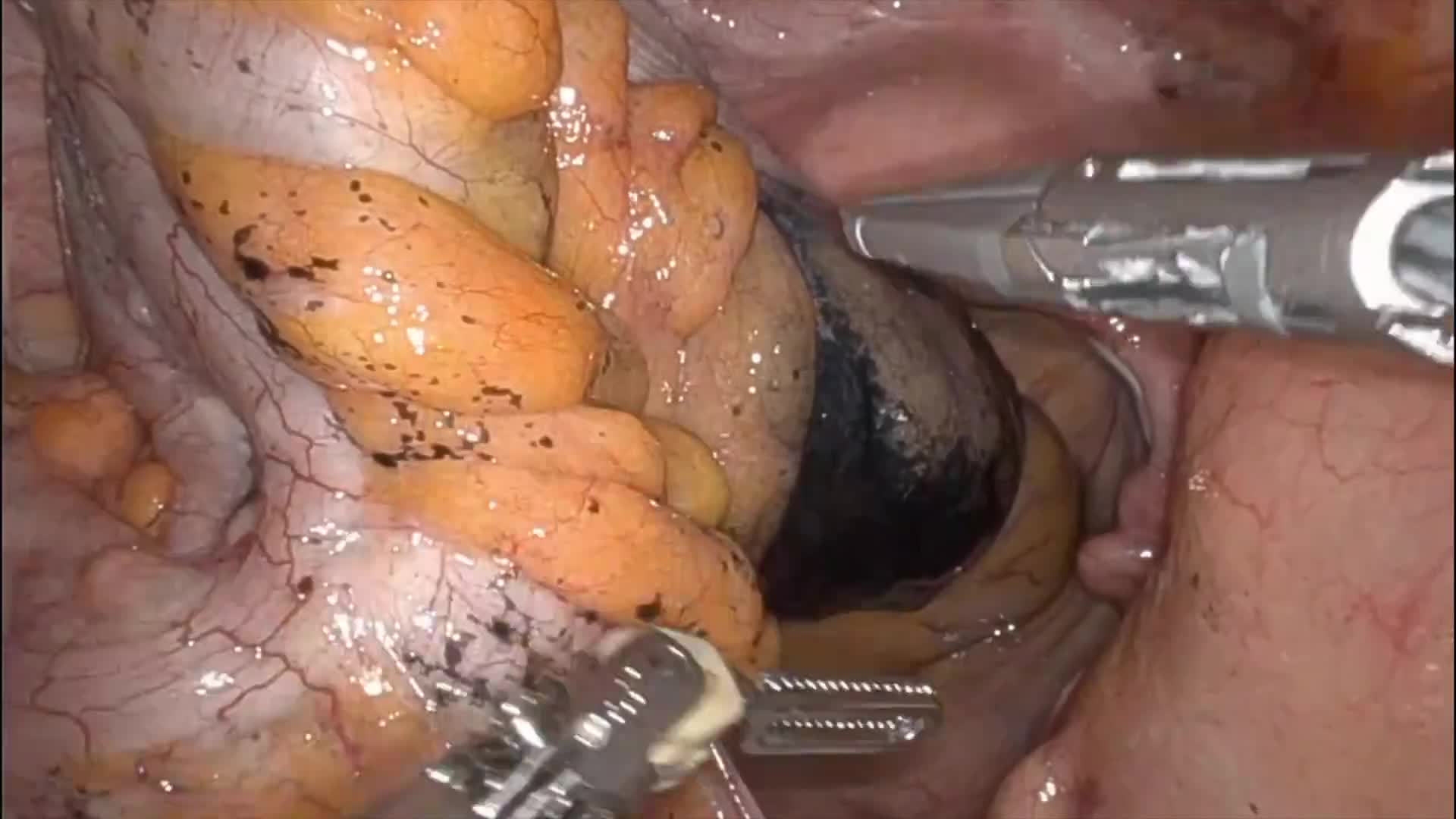
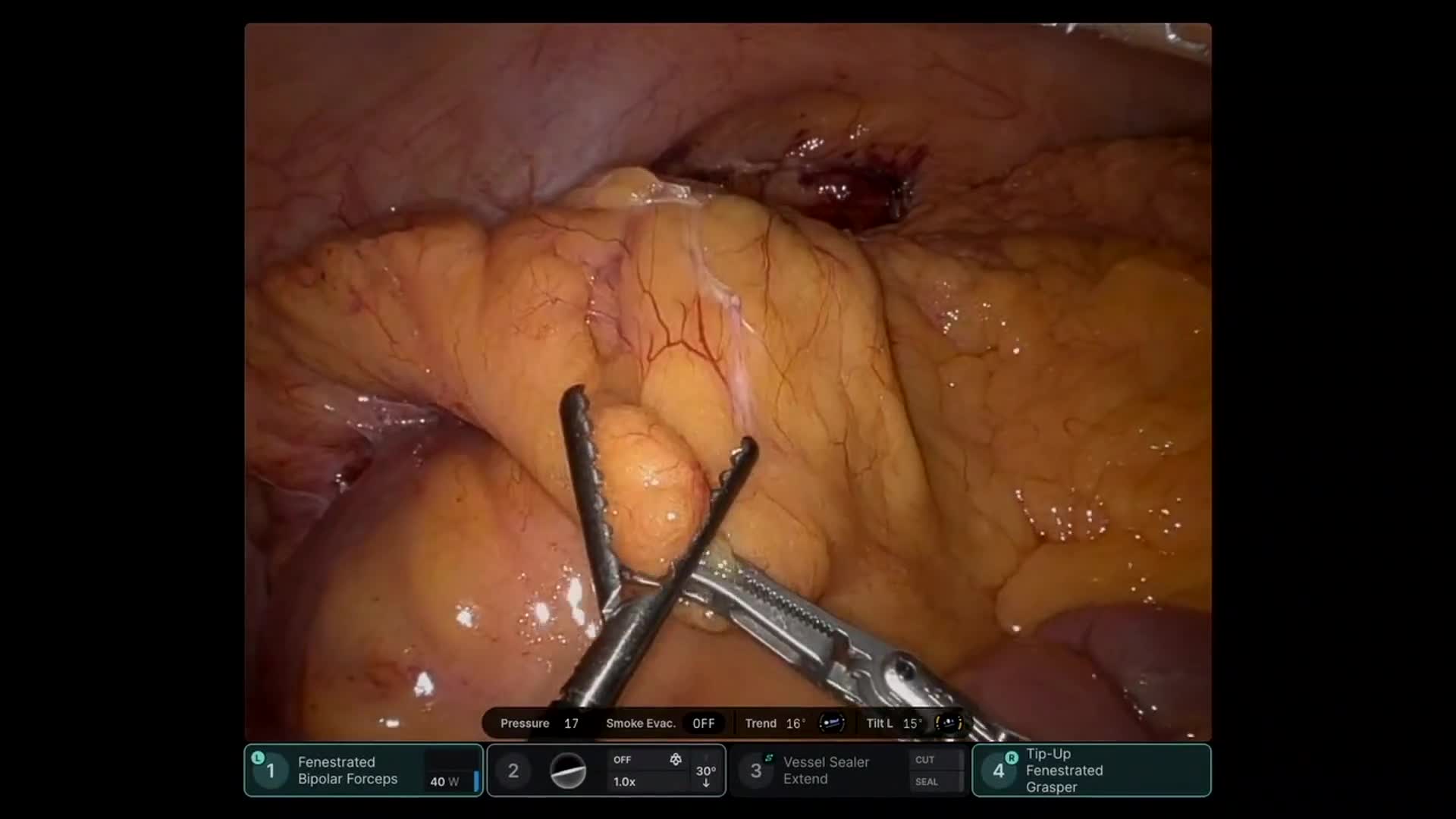
Robotic staging laparoscopy demonstrated no peritoneal metastatic disease. Intraoperative ultrasound localized a 2 cm lesion within the superior–posterior aspect of the pancreas. The lesion was carefully enucleated from the pancreatic parenchyma, and regional peripancreatic lymphadenectomy was performed.
Final pathology demonstrated a well-differentiated grade 1 pancreatic neuroendocrine tumor (Ki-67 ~1.3%). Importantly, the tumor was surrounded by pancreatic parenchyma without associated lymphoid tissue, supporting the interpretation that the lesion represented a primary pancreatic neuroendocrine tumor rather than nodal metastasis. Five additional lymph nodes were negative for malignancy.
This case illustrates the diagnostic complexity of neuroendocrine tumor staging, and demonstrates robotic techniques for suprapancreatic exposure, intraoperative ultrasound–guided localization, pancreatic tumor enucleation, and regional lymphadenectomy.